Large odontogenic tumor in Congo
Gottfried Lemperle, Christoph Sachs, Katja Kassem-Trautmann, Carsten Schröder, Jörg Kalla
The 4th Interplast Hospital in Goma, Congo
Gottfried Lemperle
Project for a 4th Interplast hospital in Goma, Congo
Gottfried Lemperle
Extreme skin tumors and burn contractures in Congo
Katja Kassem-Trautmann, Plastic Surgeon, Zug, Switzerland
Simultaneous reconstruction of the entire upper and lower lip during a humanitarian surgical mission in Africa
Arthur Charpentier1, Gottfried Lemperle2
Report 6
###
Report 7
###
Bericht 8
###

1Plastic Surgery, Wolfsgangstr. 64, 60322 Frankfurt am Main. Germany
2Department of Plastig Surgery, Martin Luther Hospital, 14193 Berlin, Germany
3Plastic Surgery, Zug, Switzerland
4Department of Anesthesia, Hospital Horgen, Switzerland
5Schwarzwald-Baar Klinikum Institut für Pathologie, Germany
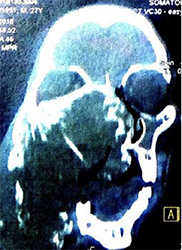
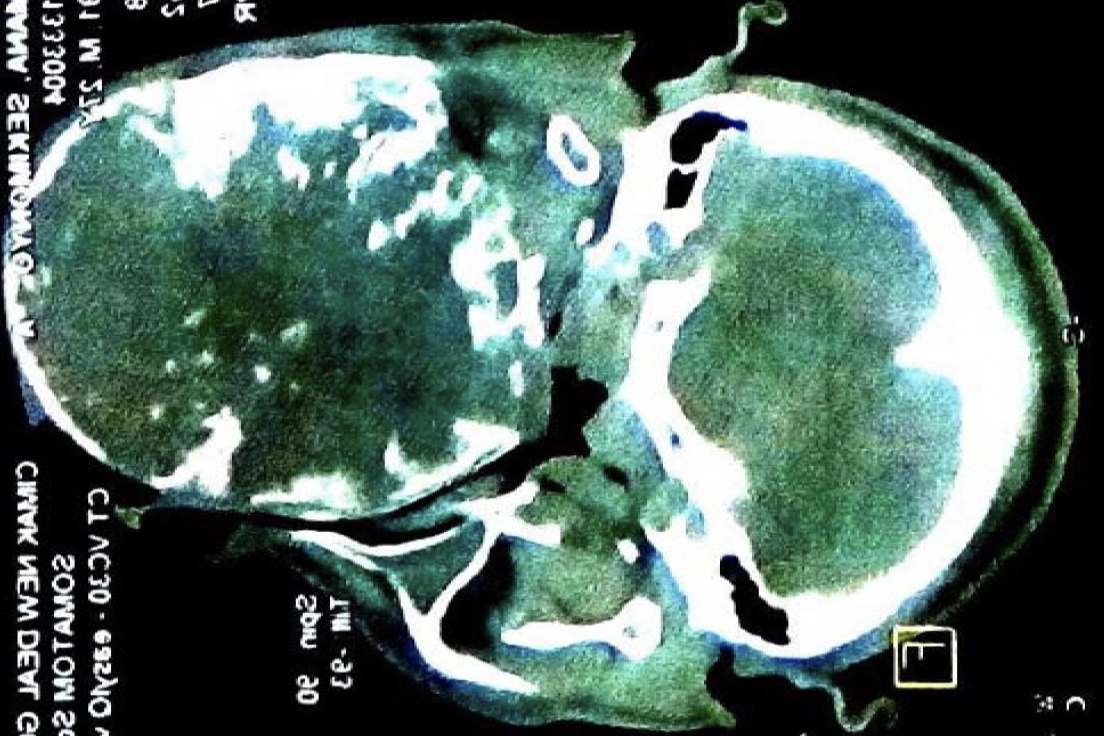
A well-developed 26-year-old male patient allegedly first mnoticed the tumor in his right maxilla 3 years earlier (Figures 1,2). His speech was slurred but understandable. Images from a Siemens Somatoma® in Goma, DRC (Figures 3,4), and CT showed space displacement from all sides, 3D reconstruction also showed bony structures within the tumor (Figures 5,6). Radiologists suspected ameloblastoma or bone sarcoma. Retropectively, however, the images also revealed the classis radiographic features of odontogenic myxoma


in which the bony trabeculae intersect at right angles ina multilocular radiolucency [3].
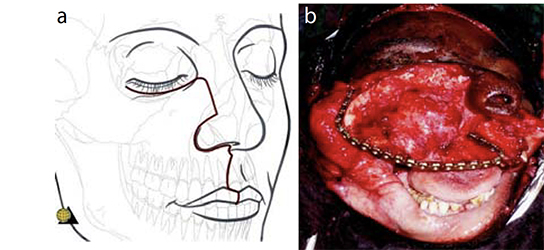
To create an osteo-myo-cutaneous pectoralis flap to reconstruct at least some parts of the patient's palate a tracheostomy was performed. Resection of the large tumor using an electric saw was relatively easy and caused no major blood loss. The now missing maxilla was reconstructed suboptimally using a metal plate that was attached in an arch shape to both zygomatic bones (Figures 7). The 5thrib, raised with the vascular pedicled pectoralis flap, was internally sawed into 4 sections and arcuately fixed with screws to the metal plate, remaining surrounded by muscle tissue [4].
The attached skin flap, which included the nipple region (the nipple was replanted) was sufficient for a tension-free closure or the "new" palate. An inner lining of the nasal side can often be omitted since, during the coming months, living epithelial cells sloughing off from nasal mucosa can be expected to epithelialize the "raw surface" of the airways. To allow optimal vascular connections to the muscle flap from the cranial side, the widely overstreched cheek skin was pressed onto the muscle from the outside with a bolus "pressure" dressing (Figures 8).
The postoperative course was without complications. The local surgeon removed the bolus dressing from the cheek after 6 weeks on the condition that the upturned pectoral muscle received sufficient vessels from the well-perfused cheek skin. Another 10 days later, he transected the osteo-myo-cutaneous pectoralis flap and discarded it.
Within the first postoperative months, there was no visible recovery yet of the extremely hyperextended facial nerve branches in the right cheek (Figure 9). The patient left the hospital dissatisfied, as his speech was now even more slurred, resembling that of an untreated cleft palate patient. Unfortuantely, he disappeared in the Congolese bush and never returned. When we wrote this article, we contacted "Heal Africa", the hospital in which a free of charge MRT and CT had been done a year before surgery, but they were unable to locate the patient. Therefore, we are unable to report on his speech, the recovery of his hyperextended facial nerve, or provide a postoperative facial X-ray. Because of the frightening appearance he had been called "the Hippoman".



The double-fist-sized tumor had a polymorphic appearance of gelatinous soft parts and solid nodules, bone trabeculae, and hemorrhages when cut through. Since the orbital floor appeared corroded from below, a 3 x 2 x 1 cm biopsy was taken from the solid white periphery to exclude sarcoma. Understandably, the local pathologist could not detect and epithelial structures. Histologic examination in Germany revealed the following truncated findings.
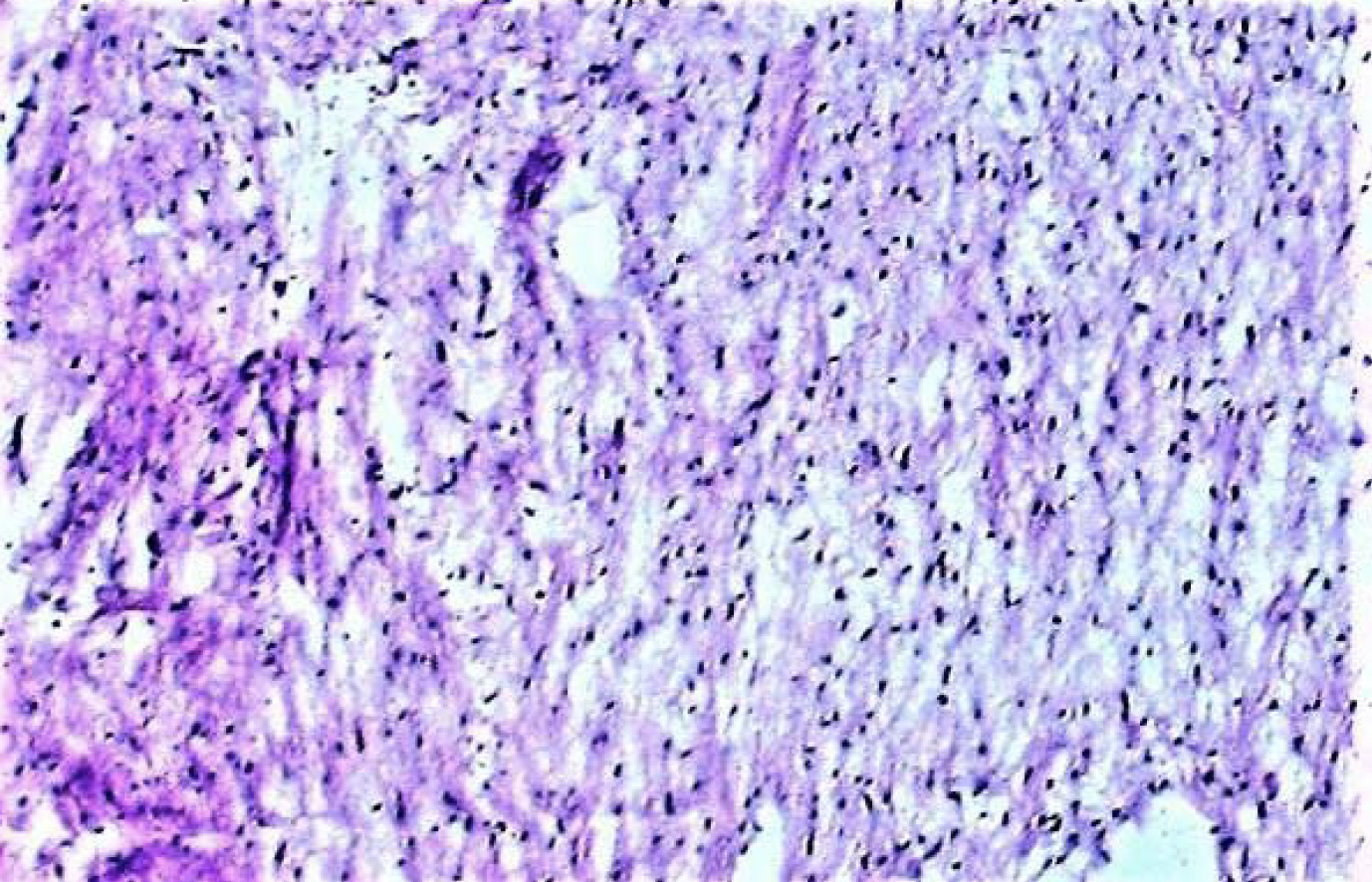
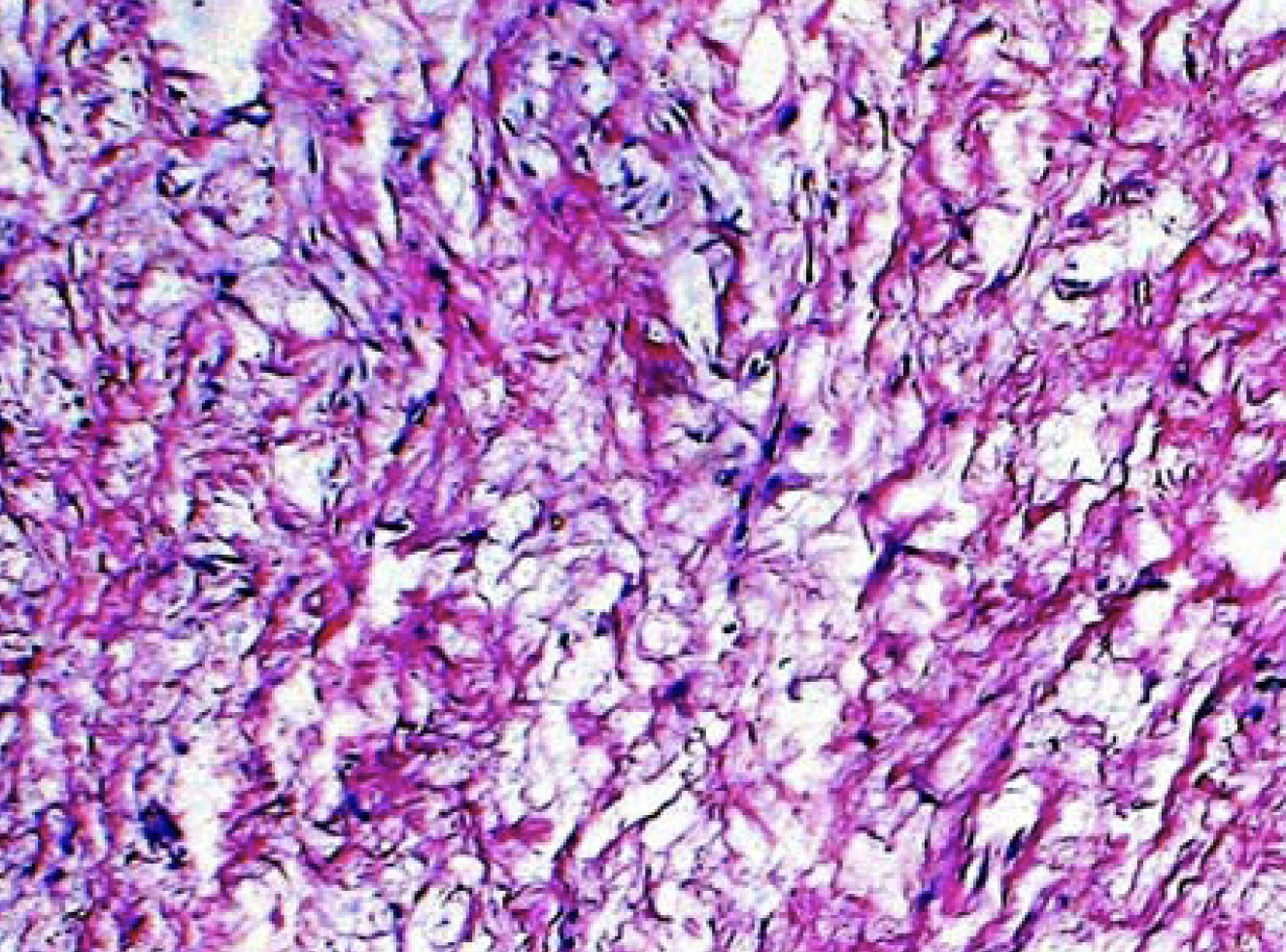
"Predominantly loosened, collagen-rich tissue with optically empty spaces as in edema. The majority had low to slightly increased cellularity with low polymorphic nuclei of fibroplasts with only sporadically recognizable nucleoli (Figure 11). No mitoses. Isolated capillary proliferates. Lipomatous structures are not identifiable. Focal calcified tissue with woven bones and single indicated lamellar structures. Loose aggregates of lymphoid cells are repeatedly found, loosely intermixed with neutrophilic segmental granulocytes, as well as single erythrocyte extravasations. Single, somewhat denser bundles of collagen fibers (Figure 12)".

Diagnosis: Depending on the clinical presentation, the findings are highly compatible with odontogenic myxoma or mysofibroma [2,3,5.6.10]
There may be a handful of maxilla-facial surgeons and plastic surgeons in the Capitals of Subsaharan Africa, who are experienced with this kind of large tumor. The pectoralis major flap was first described by Ariyan 1979 [7]. It is a pedicled myocutaneous island flap that has become the standard for soft tissue reconstruction in head and neck surgery over the last 40 years.
In the West, the described osteo-myocutaneous pectoral flap was not considered rocket science and has largely been replaced by a free forearm or even osteo-myocutaneous scapula flaps [4] had been used in our Frankfurt Department of Plastic Surgery in the early 1980s to cover devastating facial defects after noma infection in children in the Subsaharan area. In comparison with local flaps, they have the advantage of not impairing the integrity of the surrounding facial skin.

A clinical diagnosis without biopsy findings from a pathologist is always a challenge for the surgeon. Sugery is necessary to prevent future suffocation. The benignity, however, is soon obvious from the clear borders of the tumor - and if there are malignancies within the tumor, they do not influence the outcome.
In 1998, at a congress in Cape Town [8], 4,384 cases of odontogenic tumors (OT) were presented from sub-Suharan Africa: 86.9% were ameloblastoma, 6.9% were keratocystic OT, and 4.9% were myxomatous OT and 1.4% showed malignant degeneration.
Similar figures were published in Nigeria in 2016 [9]M preoperative biopsis were rarely present at the time of sugery and postoperative pathology was not always certain. i.e. complex OT was the second most common type of OT in this regard after ameloblastomas., (what was most common??)
An online revealed clinically similar-looking giant facial tumors from developing countries diagnosed as "craniofacial fibrous dysplasia", which is now considered a mutation of the gene GNAS1 on chromosome 20 [10]. A myriad of subtypes of odontogenic tumors may be considered differential diagnoses [3], most often when limited biopsies are available from "mixed" tumors [11]. For the surgeon, however, this is more of a scientific dispute with little relevance to the patient or outcome.
Africa is home to 1.3 billion people today; by 2050, the number is expected to have doubled. Most of them will have to leave their countries and flee northward. Since medeical care cannot keep up with this population explosion, we will be confronted with large odontogenic tumors much more frequetly in Europe or our humanitarian missions. Since radiacal resection is the only option for almost all adontogenic tumors, a correct diagnosis by the pathologist is clinically relevant in that 1.4% of malignancies can be identified [5] for which postoperative radiation may have to be considered. Goma, a city of 2 million inhabitants, has no facilities to offer postoperative irradiation.
The surgeion must determine the benignity of a tumor based on the clinical growth and the macroscopic sectional image during surgery to initiate further controls or therapies as necessary. The supect initial diagnosis does not always correspond to the maxim "If hooves are clattering outside, they most likely come from a horse and not a zebra" (attributed to J.F.Dieffenbach).
A clinical diagnosis without biopsy findings from a pathologist is always a challenge for the surgeon. Sugery is necessary to prevent future suffocation. The benignity, however, is soon obvious from the clear borders of the tumor - and if there are malignancies within the tumor, they do not influence the outcome.
In 1998, at a congress in Cape Town [8], 4,384 cases of odontogenic tumors (OT) were presented from sub-Suharan Africa: 86.9% were ameloblastoma, 6.9% were keratocystic OT, and 4.9% were myxomatous OT and 1.4% showed malignant degeneration.
Large irregularities after facial tumor resection are covered today with free composite flaps from the forearm or scapula. During haminitarian missions in Africa, however, there is no surgical microscope and few surgeons are used to performing anostomoses with the help of magnifying glasses. Therefore, a rather old-fashioned, but safe and reliable option is the use of a oedicled pectoralis island flap to cover most large facial defects in the reconstruction of a lost palate, and for the replacement of failed flaps [4].